A new report from Wakely Consulting Group, an HMA Company, models changes to the 2026 ACA market enrollment due to the loss of federal subsidies. Findings suggest a larger drop in ACA marketplace enrollment – lower than some feared, but higher than the CBO analysis.
Written By:
Michelle Anderson, FSA, MAAA
Chia Yi Chin, ASA, MAAA
Michael Cohen, PhD
EXECUTIVE SUMMARY:
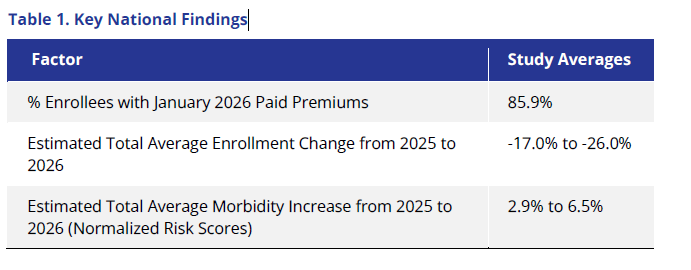
Based on unique data collection from 80% of the Affordable Care Act (ACA) individual market1, Wakely Consulting Group, a Health Management Associates, Inc., Company, estimates a material reduction in enrollment for 2026, ranging on average from 17% to 26% in total. This decrease will likely cause a deterioration in the risk pool in 2026 relative to 2025. We estimate that morbidity could be, on average, between 2.9% and 6.5% worse.
Coupled with significant changes in market composition, these impacts introduce considerable uncertainty for issuers as they develop 2027 premium rates. This report examines premium payment patterns among individual market enrollees—who paid, and who did not—in the early months of 2026 and explores potential implications for the remainder of the plan year and beyond.
The ACA individual market in 2026 experienced a significant upheaval. The expiration of enhanced premium tax credits, changes in premium tax credit eligibility as a result of recent legislation, increased costs because of high trend and inflation, rate correction from potential historical underpricing, and general uncertainty resulted in the largest net premium increase since the initial implementation of the ACA2. The general expectation is that these changes could dramatically shrink the size of the individual market. The Congressional Budget Office (CBO) projected the individual market would decline by approximately 20%, from an average enrollment of 25.4 million in 2025 to an average enrollment of 20.0 million in 20263; however, early indications from Marketplace Open Enrollment Plan (OEP) selection data are that enrollment decreased by only 5% approximately.4
So, what can we make of this discrepancy between CBO projection and OEP data? One possible explanation is that the forecasted enrollment decreases for 2026 were overstated, and the anticipated declines may not materialize. Alternatively, topline plan selection data may present an incomplete story because they include enrollees who did not—or could not—pay their 2026 premiums. If this is the case, actual attrition in the individual market in 2026 could be larger than what was reported through OEP data. The full extent of attrition in the individual market could still be forthcoming.5
Wakely conducted a unique study to evaluate the number of people who paid their first premiums across the entire individual market (both on and off Exchange) in 2026 and other corresponding market shifts. This dataset includes enrollment and premium data from participating issuers in 2025 and January 2026, representing over 30 individual markets (including two merged markets) and an estimated 80% of the total individual market.6 We analyzed January 2026 premium payment rates, shifts in market composition, and changes in member demographics. These insights enabled us to estimate potential ranges of market enrollment reductions and corresponding morbidity impacts in 2026.
Questions? Let’s ConnectKey Findings
We found that, on average, about 86% of members paid their first premium in January. This is a measurement of member premium payment compared to member enrollment, as of the end of January 2026.7 However, there was extensive variation among states. For example, among states we examined, the bottom quartile of states had an average percent of membership with paid premium of 81.9% while the top quartile had an average percent of membership with paid premium of 93.6%. States that had a higher percentage of enrollees who shopped (whether they be returning enrollees or new enrollees), and states with lower premium increases had higher percent paid ratios. In addition, on average, State-Based Exchanges (SBEs) tended to retain a higher percentage of their enrollees compared with the Federally Facilitated Exchanges (FFE) primarily driven by lower increases in member net premium, premium stabilization efforts such as state premium subsidies, Exchange operations, and more efforts on marketing and outreach.
As we consider the rest of 2026, there are factors beyond unpaid premiums that will determine the size of individual market in 2026 compared to 2025. Many enrollees exited the market at the end of December 2025. That reduction in enrollment would not be accounted for in the unpaid premium percentage. Moreover, monthly net attrition will likely look different in 2026 and could result in further enrollment losses over the course of 2026.
Using data on the percentage of paid enrollees and applying assumptions regarding average enrollment duration in 2026, Wakely is now estimating that average enrollment in the individual market could shrink 17% to 26% in 2026 compared to 2025 average enrollment, with significant variation by state, some falling much higher or lower than the potential estimated national range. State-specific characteristics are therefore key for understanding actual enrollment changes, for example, states that implemented their own state subsidy programs may be more sheltered from enrollment loss.
Beyond enrollment losses, we also found that the market composition and type of plans enrollees purchased varied in 2026 compared with 2025 (see Table 2).
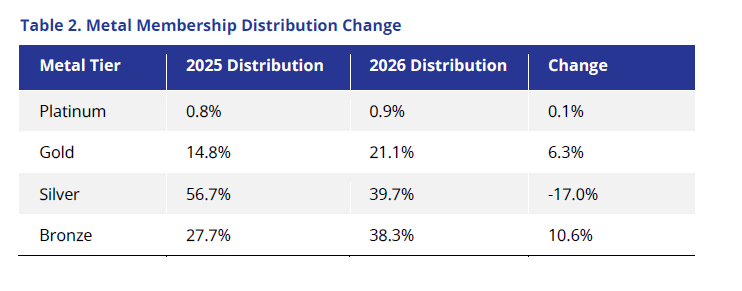
We saw extensive buy downs, with Bronze enrollment as a percentage of total enrollment expanding by almost 11% and Silver enrollment reducing by 17%. Additionally, in states where Gold premiums are lower than Silver, many of the Silver 94% members migrated to Gold plans, increasing that metal membership by 6%. This has implications, not just for consumers who could see large increases in cost-sharing8, but also for issuers who may see differences in premium levels, plan liability, and changes to risk-adjustment transfers.
Finally, given the significant reduction in total enrollment, we anticipate increases to overall morbidity. Given limited data, there are significant uncertainties associated with estimating 2026 morbidity. However given the data we have and prior research9, we estimate morbidity could increase, on average, between 2.9% to 6.5% in 2026. However this national figure may obscure the fact that some markets will exhibit very different changes in morbidity from 2025, potentially outside of the average range noted above.
There is considerable uncertainty about these results. Not only would these estimates vary, potentially significantly by state and issuer, but actual claims cost could vary even more than we estimated. Uncertainties regarding morbidity shifts and member plan enrollment could result in unpredictable and large risk-adjustment transfers, as well as dramatic shifts in claim cost spending patterns.
Changes in plan selection and market composition will cause further uncertainty in estimating 2026 financial accruals and assumption setting in 2027 premium rates. It remains a key question whether the final 2026 average premium rate increases of 26% will be sufficient, as many of the impacts were anticipated, and how issuers will react in 2027 to the estimated significant variation in rate action and potential changes in participation. It will be important to monitor emerging experience, particularly since the 2027 plan filing season is right around the corner. The following sections describe these findings in more detail, including the methodology used in the analysis, additional key findings, their implications, and the limitations of the analysis.
Download Full ReportINTRODUCTION
The Affordable Care Act (ACA) individual market experienced significant change from 2025 to 2026. Several policy changes resulted in large premium increases. The expiration of enhanced premium tax credits (ePTCs), which had been in effect for several years, expired at the end of 2025. Consequently, individuals who had received advanced premium tax credits in 2025 would see their premiums dramatically increase in 2026. For example, Kaiser Family Foundation (KFF) estimated subsidized enrollees would see their monthly premium payments increase by about 114%.10 Unsubsidized enrollees saw the largest premium hike since 2017 at approximately 26%.11
In addition to the expiration of ePTCs, other legal changes reduced Advanced Premium Tax Credit (APTC) eligibility. For example, some people with legal immigration status lost APTC eligibility and saw extensive premium increases.12
Given all of these factors, a key question surrounding 2026 was how many enrollees would retain their ACA individual coverage? If a large enrollment drop occurs, not only would there be coverage implications (i.e., a greater number of uninsured), but also potential morbidity implications (i.e., a greater proportion of sick enrollees would make up the market), which could have implications for 2027 and beyond.
PLAN SELECTIONS VERSUS EFFECTUATION VERSUS PAID PREMIUMS
The answer to how many people remain in the market depends on how and when you measure enrollment. The Centers for Medicare & Medicaid Services (CMS) has previously released data on plan selections for 2026, which showed an approximately 5% decrease in enrollment.13 However, the data CMS has released measure the “total number of people who have submitted an application and selected a plan, net of any cancellations.”14 It does not capture the number of enrollees who paid their first premium. This is an important distinction, as enrollees who do not pay their first premium would be forced to disenroll and lose their coverage. It is also important to note that an enrollee can be effectuated without paying premiums.
Enrollees who paid their premiums in 2025 or are auto-enrolled in the same plan in 2026 could count as effectuated, depending on when the data are measured.15 Effectuated subsidized16 enrollees with unpaid premiums are in a grace period. Subsidized enrollees in a grace period have 90 days to pay their premiums, after which they are retro-terminated to the start of the grace period. Consequently, effectuation enrollment numbers can shift because you can be effectuated but not have paid the owed premium (i.e., January effectuation data measured later in the year will be lower due to retro-terminations because of unpaid premiums owed).
Hence, measuring the number of enrollees who paid their premium provides a far more accurate representation of what 2026 enrollment will ultimately finalize at, which assists in analyzing and estimating the future individual market size. In reality, some of the people who currently have not paid premiums will pay their premiums and some of the people who have made partial premium payments (who we count as being paid) will not make the full payments needed to maintain coverage. Nonetheless, we think the number of enrollees with paid premiums is a reasonable approximation of what final (post retro-terminations) effectuations will resemble.
METHODS AND DATA
The analysis relied on data from the Wakely National Risk Adjustment Reporting (WNRAR) project. The WNRAR project provides Wakely with summary data from participating ACA-compliant individual market plans. Data reporting is voluntary and, thus, exclusive of some issuers in a given state. Though the data are not representative of the entire market, the WNRAR project collected data from more than 75 issuers in over 30 states and represents nearly 80 percent of ACA-compliant enrollment for the individual market.
The data include 2025 enrollment and risk score summaries from January through December 2025, January 2026 enrollment information as of February 1, 2026, February 2026 member signups from January OEP, member premium information, as well as indicators for members who paid any portion of their January 2026 premiums after APTCs were collected. Using this information, we summarized the proportion of members who had paid their premiums as of the end of January 2026. Many analyses when examining effectuation rates17 have compared the number of Exchange effectuated enrollments to the number of Exchange plan selections (i.e., numerator of effectuated enrollments and a denominator of plan selections).
Our paid premium ratio is not directly comparable because our analysis includes both on and off Exchange data and has definition/timing differences. Nonetheless, our paid members (the numerator) may be considered a reasonable approximation for what post-termination effectuated enrollment resembles. Additionally, given the measurement period, our denominator more closely resembles an early snapshot of effectuated enrollment before retro-terminations have occurred for enrollees with APTCs.
We also compared the estimated 2026 average enrollment with the average 2025 enrollment to determine a potential range in reduction in total market size. Given that the data collected for 2026 only include January member paid data, we applied a few adjustments to infer the average 2026 enrollment as follows:
- Assume that some proportion of January members with unpaid premiums will pay their premiums during the grace period and that some members who made only partial payments (and therefore counted as paid premiums) will ultimately lose coverage.
- Assume some proportion of January members with partially paid premiums, who are currently counted as having paid, will lapse due to making insufficient payments before end of the premium period.
- Assume some proportion of February member signups do not effectuate because of unpaid premiums.
- Estimate net attrition for the remainder of the year. Net attrition would include both Special Enrollment Period (SEP) additions and further terminations of enrollees covered in January and February. Historical ACA data were used as a proxy and a range was applied.
To estimate the potential range in relative level of health of the 2026 ACA market, we relied on 2025 data scored using the 2026 US Department of Health and Human Services Hierarchical Condition Categories (HHS-HCC) risk-adjustment model. Risk scores, normalized for standard demographic factors (plan metal level and CMS federal allowable rating factor age curve), were used as a proxy for relative risk of cohorts to measure the changes that occurred in 2026 relative to average relative risk in 2025.18
In addition, the standard HHS-HCC model includes a special adjustment for members who are in specific Cost-Sharing Reduction (CSR) plans. Given that members may change their plan enrollment from 2025 to 2026 due to premium differences or income changes, we have removed all CSR adjustments for risk scores for the purposes of this analysis. Although the normalized relative risk provides a reasonable approximation to morbidity, it is not a one-to-one correlation between relative risk changes and morbidity. We did not adjust for risk changes due to mix in geography.
To estimate the potential change in morbidity in 2026, we classified the 2026 enrollment into two cohorts, namely “Stayers” (i.e., members who retained the individual coverage within the same issuer) and “Joiners” (i.e., members who are new to issuers within our data collection). Note that the Joiners would have included both members who are new to the individual market as well as members who have switched their coverage. The members that left their 2025 issuer are deemed “Leavers” in this analysis. The key caveat is for the Leavers, we are unable to determine between people who switched insurers and therefore classified as Joiners, and people who ultimately dropped ACA individual coverage in 2026. Consequently, we are unable to understand the exact relative risk differences for those two cohorts.
In our analysis, Stayers retained their 2025 normalized risk scores, whereas Joiners were assumed to have varying levels of normalized risk scores based on the normalized risk scores for average market Leavers. We applied a range of assumptions to capture Joiners being 5% to 20% sicker than the Leaver population. Given that we have retained normalized risk scores year over year for the Stayer population, we have not explicitly assumed any increased acuity that would have occurred outside of changes to population mix in 2026. This is an important distinction and potentially a conservative assumption given recent increases in morbidity among Stayer populations, as reported by various sources in the industry.
We classified states into three distinct categories—federally facilitated exchange (FFE) states that had expanded Medicaid, FFE states that did not expand Medicaid, and State-Based Exchanges (SBEs)19—to determine whether the type of Exchange or state Medicaid expansion influenced results. We anticipated that the types of current enrollees and those newly entering the individual market would differ based on whether the Medicaid program included expansion enrollees. Furthermore, we anticipated that the impact would vary between FFE and SBE states because their operational processes and outreach efforts may differ. In addition, the proportion of SBE states with state-funded subsidy programs is significantly higher than in FFE states, which is likely to affect the data.
Additionally, we used Centers for Medicare & Medicaid Services (CMS) open enrollment period (OEP) data20 to analyze other potential correlations between relative risk changes and the varying enrollment cohorts. These data may be useful indicators for future changes that may occur in the Marketplace.
FINDINGS
Paid Premium Enrollment Reductions
As Table 3 indicates, on average, approximately 85.9% of January members had paid their premiums at the time of our data collection. As noted above, this ratio represents members who have paid at least a portion of the premium after APTC divided by January enrollment, at the time of the data collection. Although some of these individuals may ultimately pay their premiums, given the size of premium increases, it is likely that the vast majority of these enrollees that have not yet paid will ultimately drop their coverage in 2026.
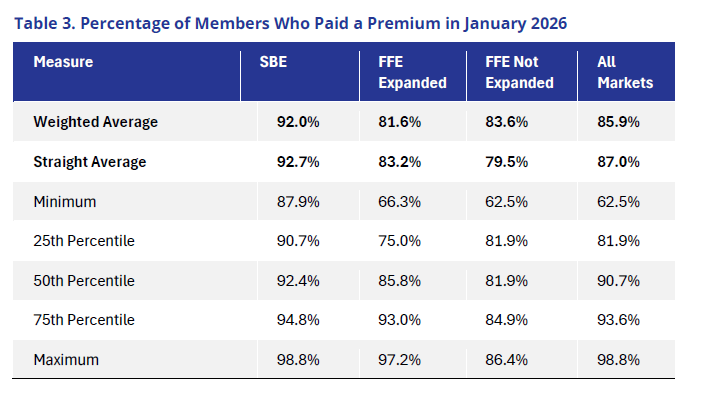
It is important to note the amount and potential reasoning for variation in payment rates. The data Wakely collected showed that the 25th percentile was approximately 82% of paid premiums, and the 75th percentile nearly 94% of members paid their premiums. This variation is even more pronounced depending on the type of Exchange and if the state had expanded Medicaid. Generally, SBE states had a higher proportion of members who paid premiums. Many SBEs had state subsidy programs and extensive outreach programs, which likely improved member retention. There are currently 10 state subsidy programs in the individual market.21 All 10 of these states are also SBEs. Several of these states have substantial state subsidy programs. For example, New Mexico’s state subsidy program fully offsets the reduction in federal subsidies for 2026.22
Conversely, FFE states had a lower percentage of members with paid premiums than SBE states. Within FFE states, most states that expanded Medicaid on a straight average basis, saw more members paying premiums than did FFE states without Medicaid expansion, although the difference between the two was insubstantial, and a number of FFE Medicaid expansion states had high premium payment rates.
Given the variation between states, the reasons for lower percentage of paid premiums are likely extensive. We found two interesting correlations we believe merit discussion and continued monitoring.
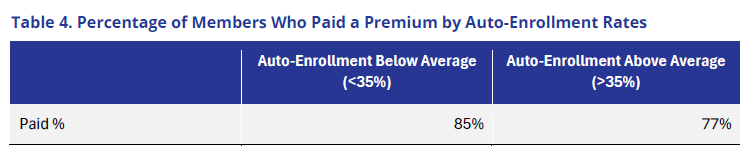
First, states with lower automatic reenrollment rates had higher payment rates, whereas states with an above average share of auto-enrolled members23 in their Exchanges (based on an average rate of 35% from OEP data) had higher payment rates. (see below).
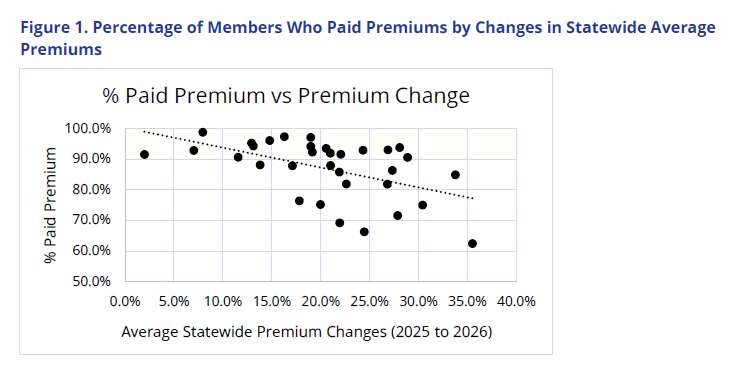
Second, we found a striking correlation between the percentage of members with paid premiums and the change in state average premiums. The higher the premium, the lower the percentage of members who paid their premium. This correlation may be true for multiple reasons. One is that higher premium increases may be driving up premiums for unsubsidized enrollees. It may also be indicative of a different benchmark plan in 2026, which could yield higher net premium increases for subsidized enrollees who did not shop when the ePTCs expired. It may also indicate that issuers correctly priced for large enrollment drops, and therefore states with high premium increases are aligning with large enrollment decreases.
Market Enrollment Reductions
Members with unpaid premiums are only part of the story in attempting to understand changes in enrollment between 2025 and 2026. Other factors to consider include:
- Some members left the market before the start of 2026 and, therefore, were excluded from the percentage of members who paid their premiums.
- States gained members from January Open Enrollment who had February start dates and were not included in paid premium calculations.
- Some members with unpaid premiums may ultimately pay their premiums and maintain coverage; conversely, some members who paid their first premium will exit the market over the course of 2026.
- Some new members will join the market through SEPs over the course of the year.
Consequently, there is considerable uncertainty about final enrollment in 2026, even with the availability of detailed January data. Nonetheless, we have arrived at a wide range of plausible scenarios, as displayed below. In the low scenario, we assumed that net attrition patterns would resemble pre-ePTCs (specifically 2019) over the course of the year. For the high scenario, we assumed that net attrition patterns were worse than 2019, given the high net premium increases and significant reduction in number of people with $0 net premiums. It is possible that with buy downs to Bronze and state subsidy programs, that more enrollees may stay covered in 2026 compared to 2019. Alternatively, it is possible that given the high net premium increases, further enrollment losses will occur, beyond even our increased net attrition. The low does not represent the lowest scenario and the high does not represent the highest scenario, but instead realistic sensitivities of potential 2026 enrollment changes.
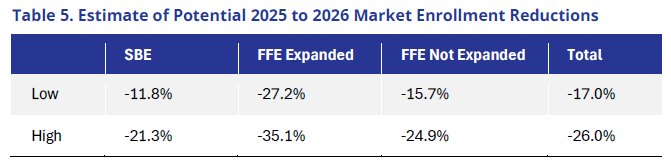
Overall, the individual market does appear to be trending toward a significant contraction in 2026 and may well resemble CBO estimated reductions.24 SBEs on average will likely experience the lowest rates of market enrollment reductions, while FFEs, especially those that expanded Medicaid, could see large declines.
Although this data collection has limits on granularity, data from CMS’s 2026 Open Enrollment public use file appears to indicate enrollees with incomes at 100% to 138% of the federal poverty level (FPL) were less likely to drop their coverage. (This cohort would be heavily subsidized and have the potential to still have a $0 net premium if they bought down to a Bronze plan.) Because FFE states that did not expand Medicaid have a higher proportion of low-income enrollees, they may have fewer enrollment reductions. It is important to note that even within these categories there is significant variation by state. Nonetheless, overall, these numbers indicate that the recent changes to subsidy structures and eligibility are, in fact, having a negative impact on enrollment.
Beyond the topline enrollment changes, there are also significant changes to market composition. The next section examines some of key changes observed in the individual market composition.
Download Full ReportMarket Composition
There were notable changes to member demographics and their enrollments between 2025 and 2026. Table 6 below analyzes the proportion of members who stayed with their issuer (Stayers) from 2025 to 2026 and what metal tier was selected compared to members who left their issuer (Leavers) at some point in 2025 i.e., left the ACA market entirely or switched issuers.
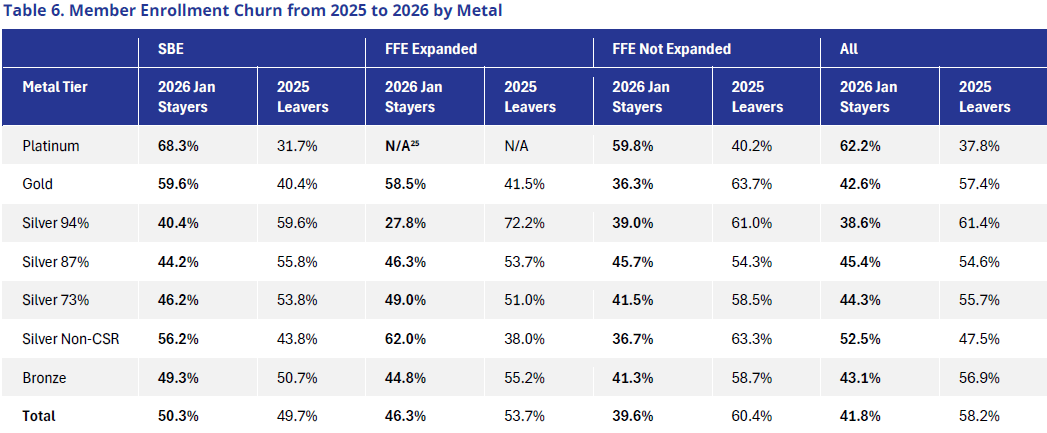
SBE states experienced less member churn, which is likely a function of many factors, including less market enrollment droppage on average and less dramatic shifts in 2026 market premiums in total and by issuer. SBE statewide average premiums increased 14% from 2025 to 2026, whereas premiums in FFE states went up 27%. In addition, many states have implemented stabilization programs such as state-based premium subsidies, which mitigate the effects of recent policy changes and corresponding net premium increases.
Churn was relatively high, particularly among Silver 94% plans, in both SBE & FFE expansion states. This finding indicates that members with lower incomes can no longer afford coverage and are dropping out of the market or are switching to cheaper plans to remain in the market. It is important to note that many of these individuals likely paid $0 or a low net premiums in 2025, so with the ePTC expiration, they had a higher incentive to actively shop for a different plan.
In analyzing how member metal tier selections changed on average between 2025 and 2026, we also observed some interesting trends. Table 7 below shows the metal tier mix for both years, segmented based on states where Gold premiums are higher than or lower than Silver, on average, in 2026.
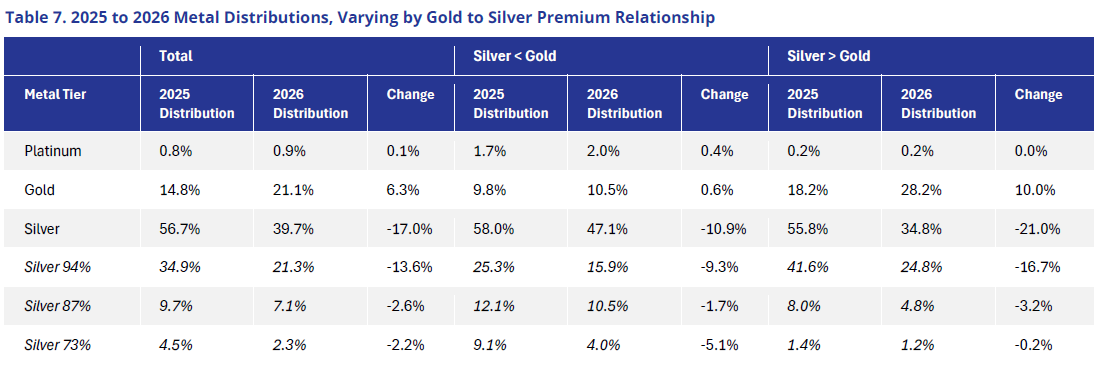

Overall, the market experienced a significant (17%) reduction in Silver membership, with 14% coming from Silver 94% CSR members, a marginal increase in Gold (6%), and a larger increase in Bronze plans (11%). The increase in Gold was mostly experienced in states where Gold premiums were less than Silver, indicating the high propensity of members buying down to plans with less generous cost-sharing to save on premiums.
We further analyzed the increase in Bronze and Gold membership resulting from members “buying down” (i.e., purchasing a plan with higher potential cost-sharing at a lower premium cost). Studies have shown that members often select plans that result in higher out-of-pocket costs than if they had selected a plan that better aligned with their expected health costs.26 This outcome may prove especially true in 2026 when an individual’s health spending may significantly affect whether the decision to buy down to a Bronze plan will ultimately produce savings.27
Table 8 below shows the propensity of buy downs by varying cohorts. We have analyzed the proportion of members buying Bronze plans in 2026 when they initially enrolled in either Silver or Gold plans. Additionally, in states where Gold premiums are cheaper than Silver’s, we have analyzed how many Silver members have purchased a Gold plan instead (i.e., likely forgoing a higher CSR actuarial value [AV] plan for premium savings). The table only includes the Stayer cohort of membership.
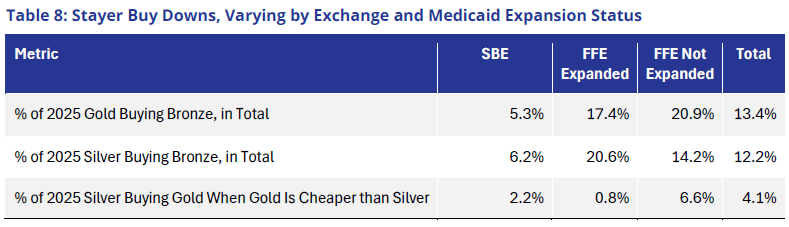
Table 9 below shows the shift in the age of the population cohorts. The allowable rating factor (ARF) is a proxy for the average age of the population, as measured under the CMS risk-adjustment factors.
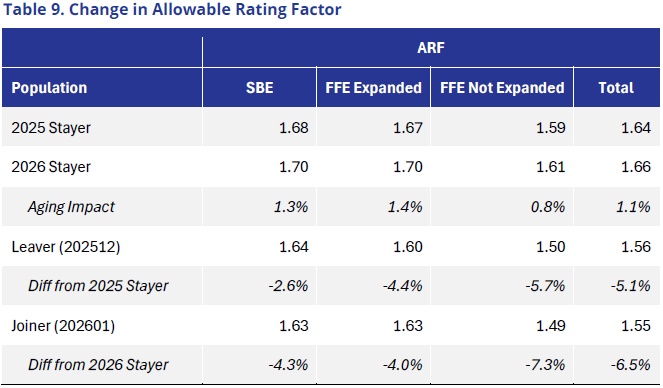
Though perhaps not a new phenomenon, Table 10 confirms that younger people are more price sensitive and will drop or shop for new coverage to potentially save money. To the extent this continues or increases in propensity, a higher risk remains of young people leaving the market if prices keep rising and thereby potentially increased morbidity rates.
Finally, the tables below analyze the change in the Statewide Average Premium (SWAP) over the past few years. Percentages for 2022 through 2025 are summarized based on national CMS Risk Adjustment Report data.
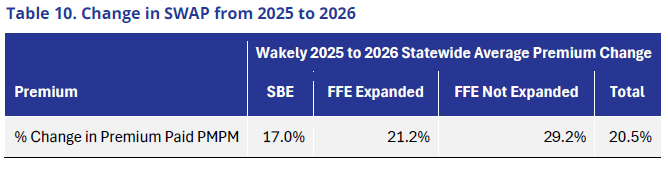
Table 11. Historical SWAP Change28, 2022–2025
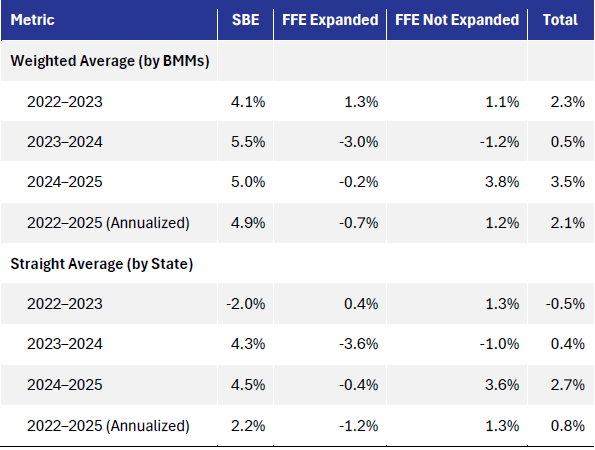
SWAP has increased dramatically in 2026 from previous years. This spike, in turn, creates a big swing in issuer transfers given that SWAP is applied on a multiplicative basis. With the same relative risk, issuers in a payable position will spend significantly more per member per month (PMPM) and vice versa, illustrating the importance of this assumption and potential misestimation in financial accruals or in future premium rate pricing estimates.
Understanding the sensitivity and risk in this assumption is critical. For example, an issuer with a $150 PMPM payable in 2025 and 30,000 members would pay $4.5 million in 2025. Under an average SWAP increase of 20.5% in 2026, that rises to $5.4 million. If the market experienced a historical average of 2.1% in 2026 instead, the payable amount would drop to $4.6 million—an $800,000 decline.
The impact of metal level selections, member buy downs, and average demographic changes have significant effects on market composition and ultimately financials and projected costs for issuers.
- The reduction in Silver CSR members may affect the amount of cost-share subsidies that issuers reimburse for members and the corresponding load included in the Silver premium rates. Issuers will need to consider the implications of their ultimate member distribution and overall change to Silver costs resulting from these shifts.
- Given that the level of APTC members receive is tied to the second lowest cost Silver plan, if Silver premiums reduce as a function of fewer lower income members enrolled in CSR plans, the result may be an increase in member net premium and compounding impacts on enrollment drops, buy downs, and morbidity.
- As membership selections change, so will the morbidity of members in each plan and metal level. For example, data have shown that lower income members enrolled in Silver CSR plans who shift down to Gold are healthier on average than those that remain. Further, the composition of Bronze membership will likely change. Because morbidity among members varies by plan, it will have a variety of implications such as impacts on risk-adjustment transfers by metal level, the use of services by cohort, and actual AVs by plan. It will be increasingly difficult to benchmark emerging experience against historical expectations.
- As noted above, risk-adjustment calculations are a function of the SWAP (i.e., multiplicative scalar to ultimate transfers). While issuer premium rate changes highly impact that number, plan selections and member demographics must also be considered. Given significant shifts in metal level, age, and what issuers members select, there is uncertainty regarding the ultimate SWAP. The higher the SWAP, issuers pay more and receive more, all else equal.
Morbidity and Pricing Considerations
The above findings highlight several important considerations, although one of the most uncertain and difficult to predict implications is the relative morbidity of the members who remain in the market in 2026. Members that are new to issuers in 2026 do not have sufficient claims at present to create risk scores.
Wakely used a simplified model to estimate morbidity change using normalized risk scores described in the Methodology section. This model blends the normalized relative risk of members who are retained by issuers in 2026 (Stayers) with new enrollees to an issuer (Joiners). Given that we are unable to determine the risk of the members who ultimately dropped coverage from their insurer in 2025 and who enrolled with a new issuer in 2026, we sensitivity tested assumptions for the relative risk of Joiners by assuming those forgoing coverage are healthier than those remaining.
We assumed that Joiners (members who switched issuers or newly enrolled in 2026) will be 5% to 20% sicker than the 2025 Leaver cohort (members who dropped coverage or switched issuer in 2026) to reflect the phenomenon that members who choose to pay higher premiums are more likely in need of healthcare coverage and sicker than those leaving.29 Table 12 below shows the averages of state experiences under the low (5%) and high (20%) scenarios.
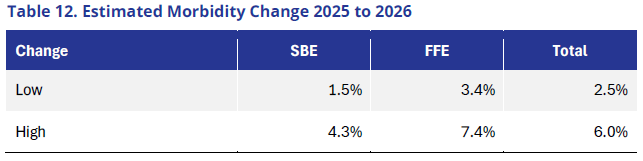
This simplified estimate showed that morbidity changes due to population acuity, from healthier members leaving the market, are between 2.5% and 6.0% in 2026, with FFE states having higher increases. Note that this model does not assume any worsening of risk in the Stayer population. Therefore, actual impact of morbidity may be higher than we estimated. In addition, the modeled results also varied significantly by individual state.
In addition, we estimated the difference in morbidity between Stayers who paid and Stayers who did not pay their January premiums. We found the aggregate morbidity of paid Stayer members is about 10.2% higher than among unpaid members. On a state-by-state straight average basis, the paid Stayer members’ estimated morbidity is 6.2% higher than unpaid Stayer members. In other words, those members with paid premiums tend to be sicker than those members with unpaid premiums, for whom we have risk score data. While there is considerable state-specific variation, the data suggest that individuals exiting the market are generally healthier.
According to the Kaiser Family Foundation, issuers, on average, expected an approximately 4% increase in rates because of worsening morbidity as a result of the expiration of ePTCs in 2026.30 As we consider forthcoming changes to 2027 premium rates, issuers will be examining their data to determine whether their 2026 rate increases were sufficient. As the above table illustrates, in some cases the rate increases may have been sufficient, but in others, may have been too low, which could produce additional pressures on rate filings in 2027 beyond the additional increases that will need to be considered. Possibilities include further policy changes and medical cost trend, which has been higher than normal in the ACA market in recent years. A key remaining question is whether the final 2026 average premium rate increases of 26%31 will be sufficient, as many of the impacts were anticipated, but all of these factors combined could contribute to compounded rate increases.
Please refer to the Key Limitations section for a full listing of important considerations and caveats associated with the changes in relative risk scores and what factors may be contributing to the increases.
CONCLUSION
2026 marks a significant shift in the structure of the individual market, driven by changes to premium tax credits and other regulatory factors that have led to substantial—and highly variable—premium rate changes. As issuers prepare 2027 rate filings, a key question is how enrollment has evolved in 2026 and how market morbidity is changing, particularly given the likelihood of continued market contraction and further shifts in 2027. Additionally, how states respond with policies and operations to influence enrollment changes are equally important.
Data collected by Wakely indicates that these policy changes are already having a pronounced impact across nearly all aspects of the individual market, including enrollment levels, market composition, and morbidity. At the same time, data limitations underscore the ongoing uncertainty surrounding both 2026 experience and future market conditions. As a result, monitoring enrollment trends and risk scores is especially critical this year.
Despite current concerns around risk pool deterioration and uncertainty, it is important to recognize that the ACA individual market has experienced periods of volatility throughout its history. Many recent changes effectively reverse policies implemented in previous years, and enrollment patterns may begin to resemble those seen in earlier phases of the ACA. Although enrollment declines are expected, total 2026 enrollment will almost certainly remain above 2019 levels, prior to the introduction of enhanced premium tax credits.
Looking ahead, the ACA Individual Market’s ongoing sustainability will depend on several factors, including issuers’ ability to price premiums adequately, regulatory efforts to support market stability, and the continued use of evolving tools and analytics. For 2027 rate development, issuers will need to consider not only 2026 enrollment experience, but also broader factors such as trend changes, emerging utilization patterns, and other market dynamics.
Wakely intends to publish additional research on this topic later in the year as more data become available.
Download Full ReportKEY LIMITATIONS
This paper is provided for public informational and educational purposes only. Wakely and the authors of this paper were not funded by any Principal in the preparation of this whitepaper. Using the information in this report for other purposes may be inappropriate. We do not intend for this paper to be relied upon by external parties. Please retain your own actuarial experts to interpret the results and review your market-specific results, if they are available. Users of the results should be qualified and understand the inherent uncertainty. Actual results will vary, potentially materially, from the estimates included within this report. Wakely does not warrant or guarantee the projected values included in the analysis. Any distribution of the information in this paper should be shared in its entirety.
Chia Yi Chin and Michelle Anderson are the actuaries who coauthored this paper. Chia and Michelle are Members of the American Academy of Actuaries. Michelle is a Fellow of the Society of Actuaries, and Chia is an Associate of the Society of Actuaries. They meet the Qualification Standards of American Academy of Actuaries to issue the analysis herein. Michael Cohen, PhD, also contributed significantly to this report.
Wakely provides actuarial services to a variety of clients throughout the health industry. Our clients include commercial, Medicare, and Medicaid health plans, the federal government and state governments, medical providers, and other entities that operate in the domestic and international health insurance markets. The authors here are financially independent and free from conflict concerning all matters related to performing the actuarial services underlying this analysis.
Wakely does not make any endorsement, representation or guarantee with regard to any content, and disclaim any liability related to the use or misuse of any information provided herein. This article should not be construed as professional or financial advice. The opinions and estimates included in this report are those of the authors and may not represent those of other Wakely actuaries. Following are the key limitations of this analysis.
- Limited months of data. The analysis was based on January through December 2025 data, January 2026 enrollment data, and February 2026 enrollment data. With any analysis involving emerging experience, it is important to consider associated caveats and the range of plausible outcomes with incomplete data, as the annual completion will vary year over year.
- Risk score to claims correlation. The Department of Health and Human Services Hierarchical Care Categories (HHS-HCC) risk-adjustment model offers an imperfect approximation of morbidity. Risk scores are calculated based on member-level demographic (age and sex), medical, and pharmacy data. They are influenced by a variety of factors, including morbidity, claims volume, accuracy of coding and documentation, member engagement, data integrity, etc.
- Coding trend. Members’ risk scores are expected to increase yearly based on their established care network, patient history, coding documentation, and other factors. For this study, we did not include any coding trend as we relied on 2025 risk scores for both the 2025 and 2026 average morbidity rates. Adjustments to risk scores were applied only to reflect the changes in age and plan selections. To the extent that future studies use 2026 actual risk scores, coding trend would be implicitly reflected in 2026 risk scores.
- Membership mix. Not all membership mix changes were considered, including any shift in geographic mix by region between 2025 and 2026. In addition, the normalization of AV and ARF was based on the risk-adjustment model factors, which are an inaccurate representation of claims cost curves. To standardize the change across markets, we have adopted the federal standard ARF published by the Centers for Medicare & Medicaid Services (CMS).
- Data reliance. The information used in this study included summarized data from health plans that were reviewed for reasonableness but not audited. Any deficient data submitted may affect the results, potentially significantly. Further, the data collected are dependent on issuer participation and, therefore, not fully representative of all issuers and markets.
- Variability. The conclusions will vary by state, and any additional data will influence results as well.
ACKNOWLEDGMENTS
The authors want to extend special thanks to Niki Daul, Zimo Han, Kayla Zimdars, Zach Sherman, Karan Rustagi, Matt Fiedler, and Lisa Winter for their assistance with the analysis and earlier drafts of the report. Please contact Michelle Anderson at , Michael Cohen at , or Chia Yi Chin at with any questions or to follow up on any of the concepts presented here.
Sign up below to be the first to receive information on upcoming webinars on this topic:
Continue the Conversation- For purposes of this paper all references to the individual market should be interpreted as referencing ACA plans or for plans for whom the market reform rules impact pricing and risk adjustment transfers shift money. ↩︎
- Cox C. ACA Insurers Are Raising Premiums by an Estimated 26%, but Most Enrollees Could See Sharper Increases in What They Pay. KFF. October 28, 2025. Available at: https://www.kff.org/quick-take/aca-insurers-are-raising-premiums. ↩︎
- Congressional Budget Office. Federal Subsidies for Health Insurance. February, 2026. Available at: https://www.cbo.gov/system/files/2026-02/51298-2026-02-healthinsurance.pdf. ↩︎
- Centers for Medicare & Medicaid Services. Health Insurance Exchanges 2026 Open Enrollment Report. Available at: https://www.cms.gov/files/document/health-insurance-exchanges-2026-open-enrollment-report.pdf. ↩︎
- Subsidized enrollees with effectuated coverage get a grace period of 90 days to pay their premiums. Consequently, after April there can be substantial revisions to early enrollment numbers. ↩︎
- Data collected includes approximately 238 million member months from 2025 experience ↩︎
- Please refer to the “Plan Selections Versus Effectuation Versus Paid Premiums” section of this paper to better understand the differences in data measurement. ↩︎
- Cohen M, Anderson M, Johnson D. Member Cost-Shifting Implications of Premium Tax Credit Expiration. Association for Community Affiliated Plans. Available at: https://www.communityplans.net/research/member-cost-shifting-implications-of-enhanced-premium-tax-credit-expiration/. ↩︎
- Prior research has tended to show individuals exiting the market due to premium increases tend to be healthier than those who remain. For example: McIntyre AL, Shepard M, Wagner M. Can Automatic Retention Improve Health Insurance Market Outcomes? April 2021. Available at: https://www.aeaweb.org/articles?id=10.1257/pandp.20211083. ↩︎
- Cox C. ACA Insurers Are Raising Premiums by an Estimated 26%, but Most Enrollees Could See Sharper Increases in What They Pay. KFF. October 28, 2025. Available at: https://www.kff.org/quick-take/aca-insurers-are-raising-premiums-by-an-estimated-26-but-most-enrollees-could-see-sharper-increases-in-what-they-pay/. ↩︎
- Ibid ↩︎
- Beginning in 2026, lawfully present immigrants whose income is below 100% federal poverty level (FPL) but are ineligible for Medicaid coverage due to their immigration status lost eligibility for APTCs. ↩︎
- Centers for Medicare & Medicaid Services. Marketplace 2026 Open Enrollment Period Report: National Snapshot. January 28, 2026. Available at: https://www.cms.gov/newsroom/fact-sheets/marketplace-2026-open-enrollment-period-report-national-snapshot-2. ↩︎
- Ibid ↩︎
- Subsidized enrollees who effectuate have 90 days to pay their premiums. During this grace period they count as effectuated. If they never pay their premiums, then their coverage is retroactively terminated. Consequently, January effectuated enrollment could look different if measured in February/March than in April after the grace period expires. ↩︎
- Unsubsidized enrollees also receive a grace period, albeit the length of this grace period is determined by state law. ↩︎
- Lo J, Ortaliza J, Wager E, Cox C. ACA Marketplace Enrollment is Down in 2026—But All of the Data Isn’t in Yet. February 5, 2026. Available at: https://www.kff.org/affordable-care-act/aca-marketplace-enrollment-is-down-in-2026-but-all-of-the-data-isnt-in-yet/. ↩︎
- Normalized Relative Risk = PLRS / (AV * ARF), where PLRS = Plan Liability Risk Score, AV = Actuarial Values, ARF = Allowable Rating Factor. ↩︎
- We only included SBEs in states that have expanded Medicaid in the data presented in this report. ↩︎
- Centers for Medicare & Medicaid Services. 2026 Marketplace Open Enrollment Period Public Use Files. Available at: https://www.cms.gov/data-research/statistics-trends-reports/marketplace-products/2026-marketplace-open-enrollment-period-public-use-files. ↩︎
- Norris L. Which States Offer Their Own Health Insurance Subsidies? March 11, 2026. Available at: https://www.healthinsurance.org/faqs/which-states-offer-their-own-health-insurance-subsidies/. ↩︎
- Grisham ML, Armijo K, Smith AC, Huff KS, Kozlowski N, Flannery D. The Marketplace Affordability Program for Middle Income Households. Health Care Authority. November 18, 2025. Available at: https://api.realfile.rtsclients.com/PublicFiles/6c91aefc960e463485b3474662fd7fd2/50c9a4d0-d5c8-48aa-8b9a-5c43e8fa23bc/Addendum%201_MAP%20P%26P%20Middle%20Income%20Household.pdf. ↩︎
- Centers for Medicare & Medicaid Services. 2026 Marketplace Open Enrollment Period Public Use Files. Available at: https://www.cms.gov/data-research/statistics-trends-reports/marketplace-products/2026-marketplace-open-enrollment-period-public-use-files. ↩︎
- Congressional Budget Office. Federal Subsidies for Health Insurance. February 2026. Available at: https://www.cbo.gov/system/files/2026-02/51298-2026-02-healthinsurance.pdf. ↩︎
- Platinum enrollment was 0 according to the data we received for this cohort ↩︎
- Bhargava S, Loewenstein G, Sydnor J. Choose to Lose: Health Plan Choices from a Menu with Dominated Option. Q. J. Econ. April 27, 2017. doi: 10.1093/qje/qjx011 ↩︎
- Cohen M, Anderson M, Johnson D. Member Cost-Shifting Implications of Enhanced Premium Tax Credit Expiration. Wakely. September 16, 2025. Available at: https://communityplans.wpenginepowered.com/wp-content/uploads/2025/08/Wakely_ACAP-EPTC-Expiration-Effects_9.15-ACAP-FINAL.pdf. ↩︎
- Historical data based on CMS June 30th reports (Premium Stabilization Programs | CMS) data accessed on 4/7/2026. ↩︎
- McIntyre AL, Shepard M, Wagner M. Can Automatic Retention Improve Health Insurance Market Outcomes? April 2021. Available at: https://www.aeaweb.org/articles?id=10.1257/pandp.20211083. ↩︎
- Lo J, Ortaliza J, McGough M, Wager E, Cox C. Premium Payments if Enhanced Premium Tax Credits Expire. KFF. September 19, 2025. Available at: https://www.kff.org/affordable-care-act/premium-payments-if-enhanced-premium-tax-credits-expire/. ↩︎
- Cox C. ACA Insurers Are Raising Premiums by an Estimated 26%, but Most Enrollees Could See Sharper Increases in What They Pay. KFF. October 28, 2024. Available at: https://www.kff.org/quick-take/aca-insurers-are-raising-premiums. ↩︎


